Numan
Numan action requests
Saving £100K of operational costs a year.
About
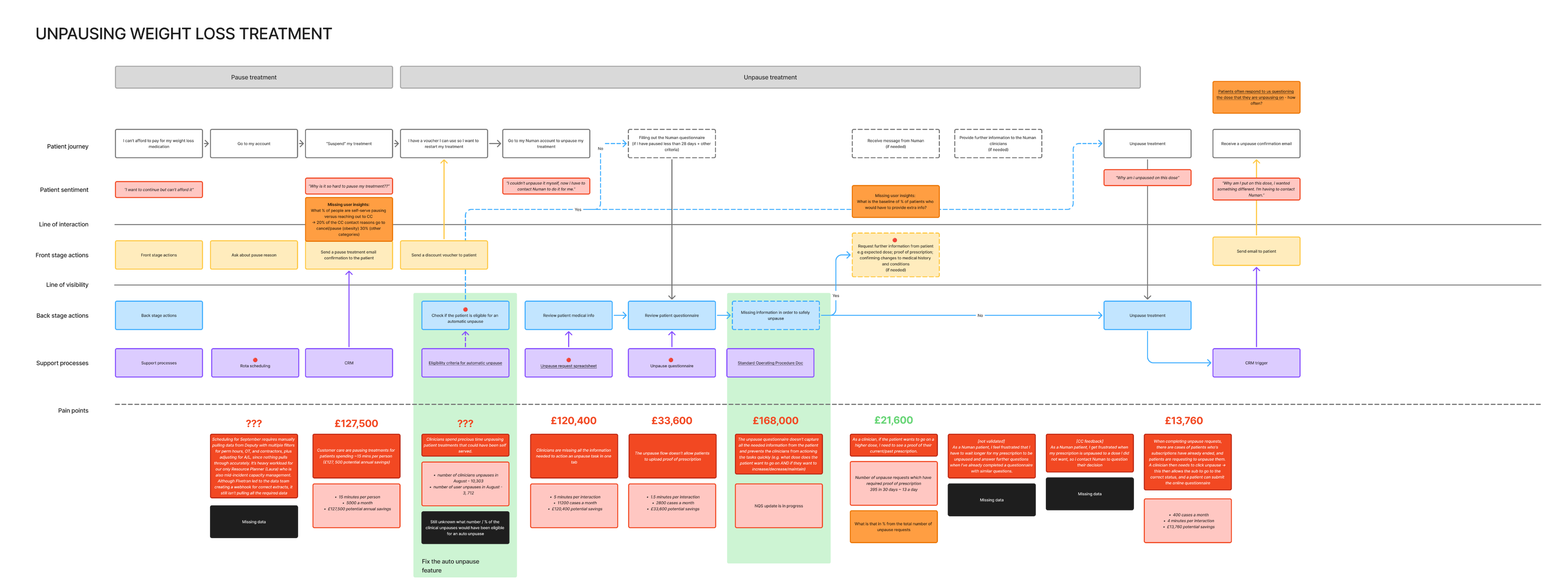
Action requests are part of a broader platform transformation - moving away from the old Electronic Health Record (EHR) and building a new one starting with the most common clinical workflows. The core problem being solved is the multi-screen navigation clinicians rely on to gather enough clinical context, with the goal of making those workflows faster, safer, and better. The first action request built was the unpause request, capturing the care plan for patients pausing and unpausing their weight loss prescription.
Key Decisions
This was an mportant decision which meant we’re showing just the right information at the right moment to clinicians to help them focus and save time.
Low fidelity gave us early confidence, high fidelity and realistic clinical data were critical in making the right UX and UI decisions.
Role playing as a patient was key to help clinicians forget about the current interface and support them in envisioning something new.
Process
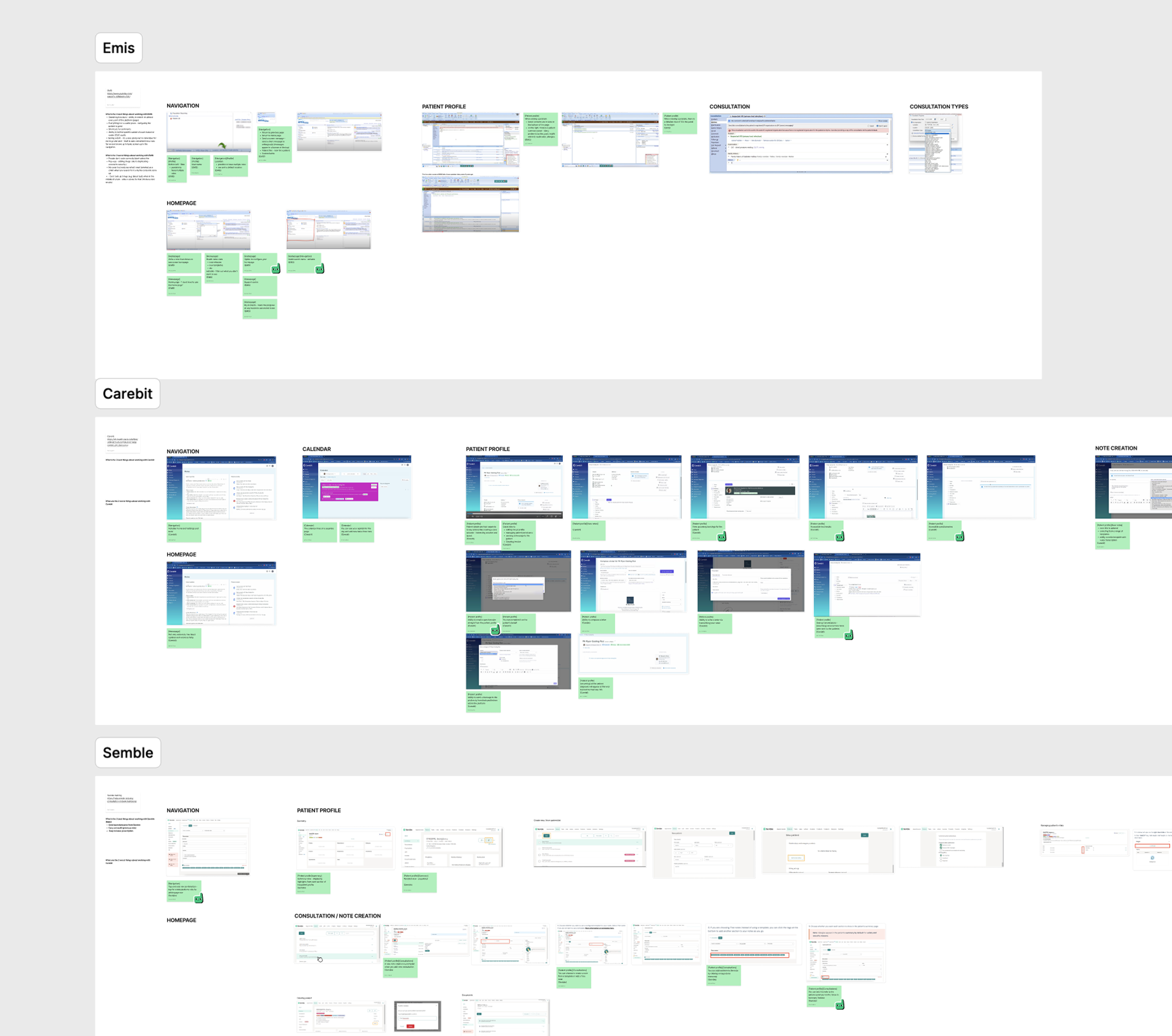
Understanding the problem space
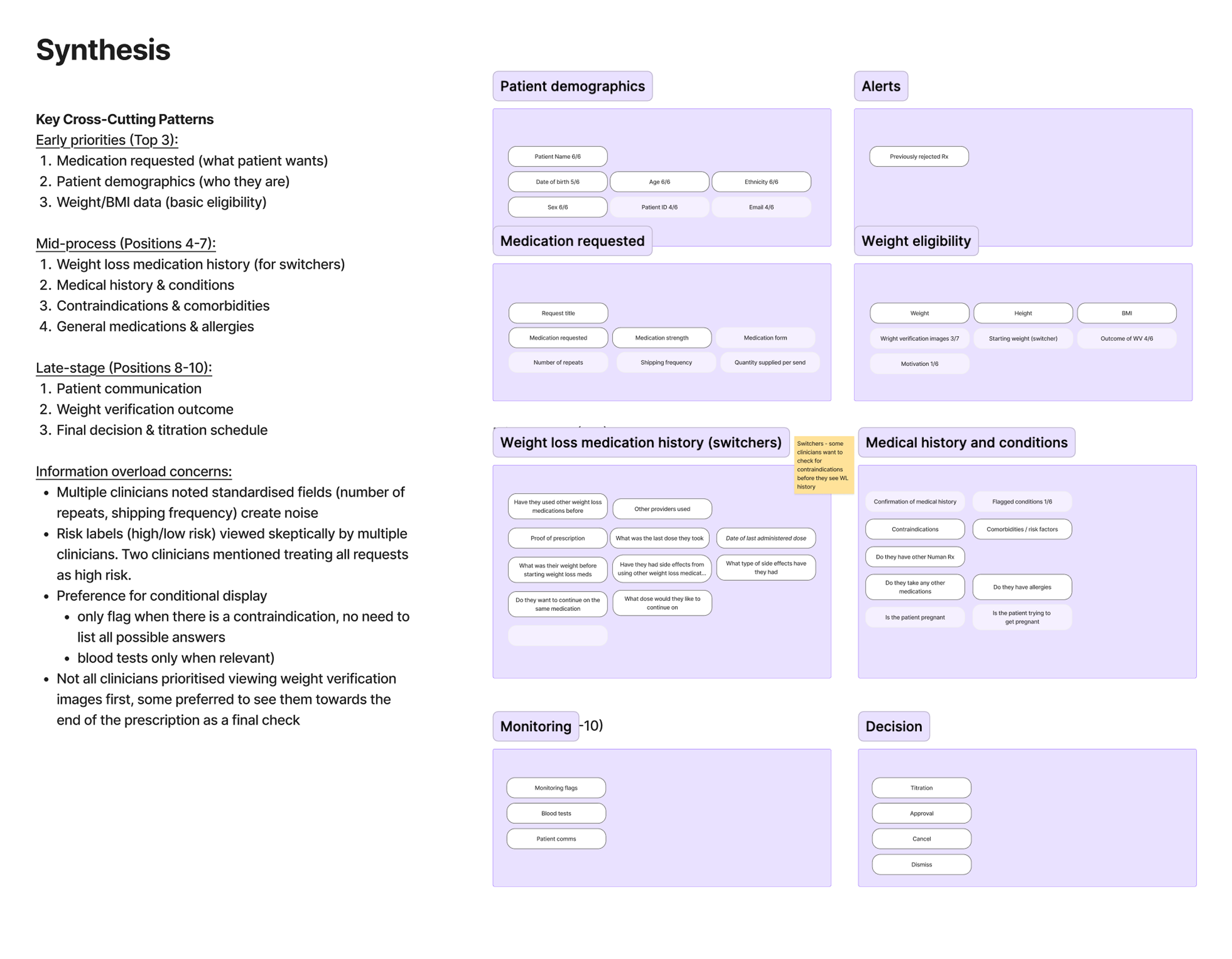
The research phase drew on several overlapping streams of work. Competitor research across other EHR platforms helped establish what good, and bad, looked like elsewhere. Shadowing sessions with clinicians - which ran in parallel with the clinical notes project - fed directly into understanding where the friction points were and the core user needs. Card sorting helped establish mental models for how content should be arranged and grouped. Workshops originally scoped around the patient profile ended up contributing significantly to this work too.
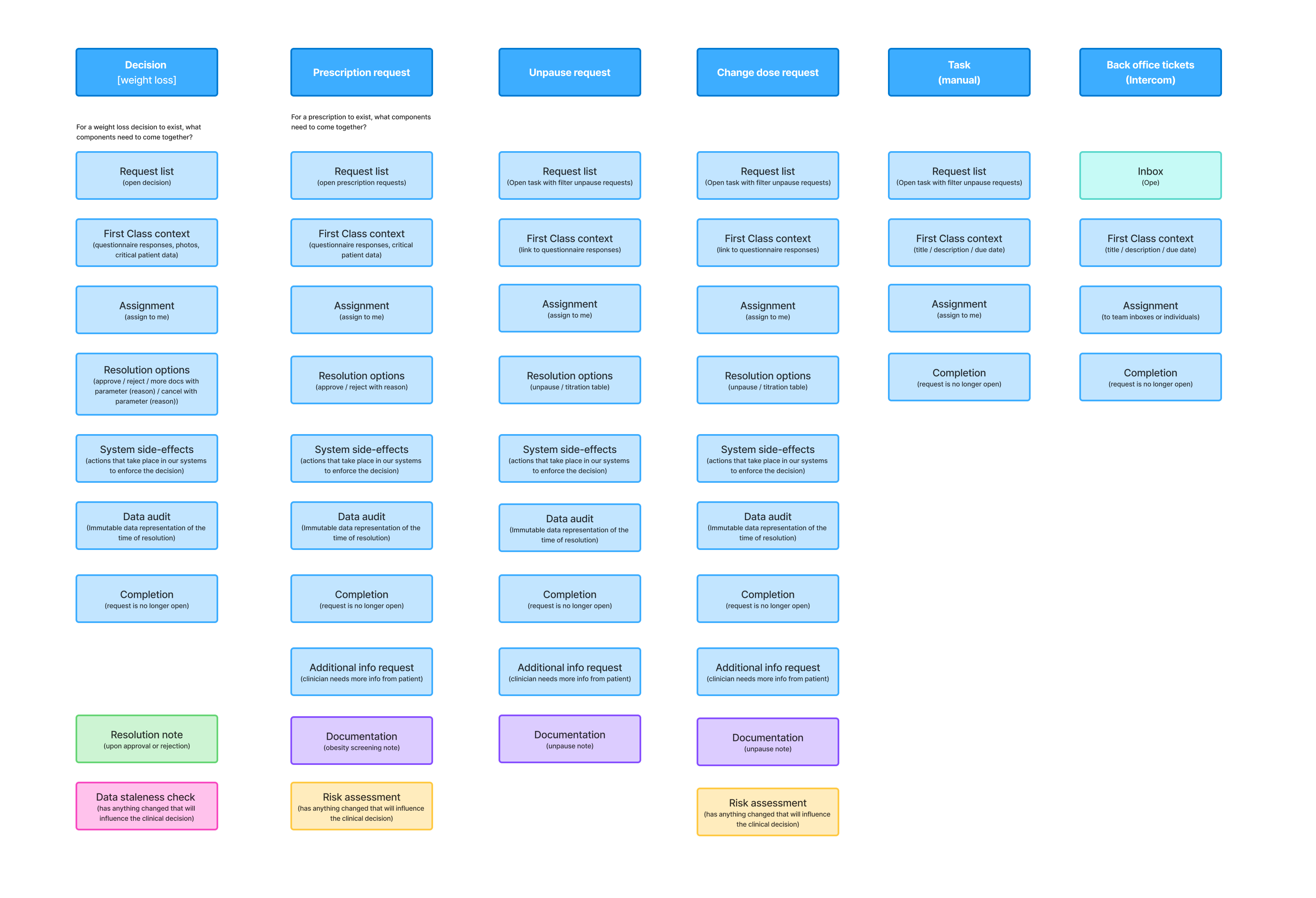
One of the most important early questions was definitional: what actually is a clinical task in the current EHR, what other clinical actions exist, and should all of these be represented by one thing in the new platform? Answering that required a series of technical discussions with the engineering team to build a shared understanding and agree on new definitions - work that shaped the entire direction of the project.
Getting clinicians to imagine something new
One of the challenges of this project was that clinicians were so familiar with the existing system that they struggled to imagine anything different. Getting them involved in ideation required more than standard facilitation techniques. In some sessions I took a more unconventional approach - I roleplayed as a patient with specific health complaints seeking weight loss medication, and asked clinicians to interact with me as if we were in a real appointment. This helped surface what information they instinctively seek first and gave me a much more natural picture of how a flow could be structured around their actual thinking rather than the legacy system.
Even with that, some needs only became visible later in high fidelity testing - when the details were concrete enough for clinicians to pinpoint exactly what was missing or what could work better. It was a good reminder that different fidelities unlock different kinds of feedback.
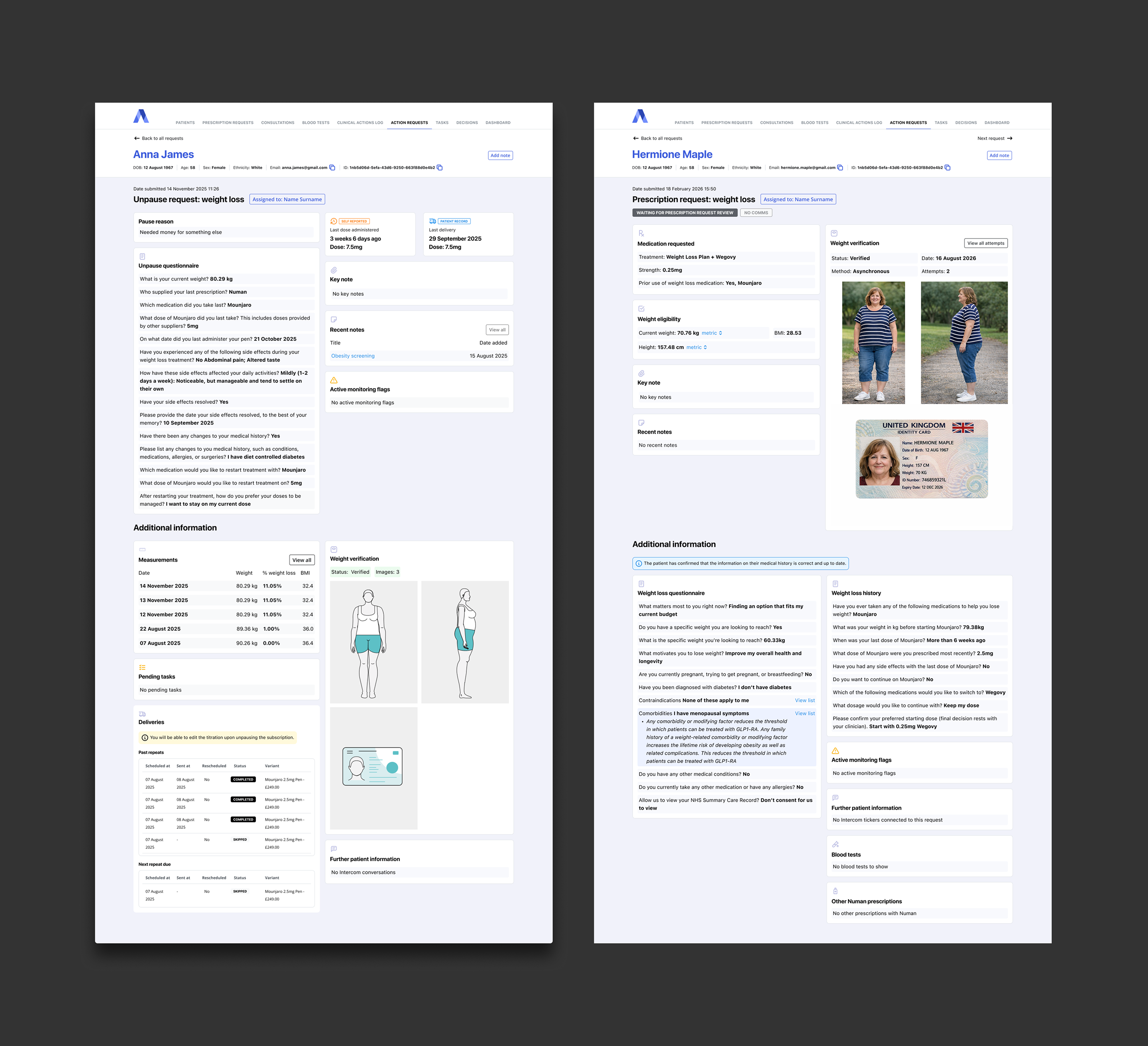
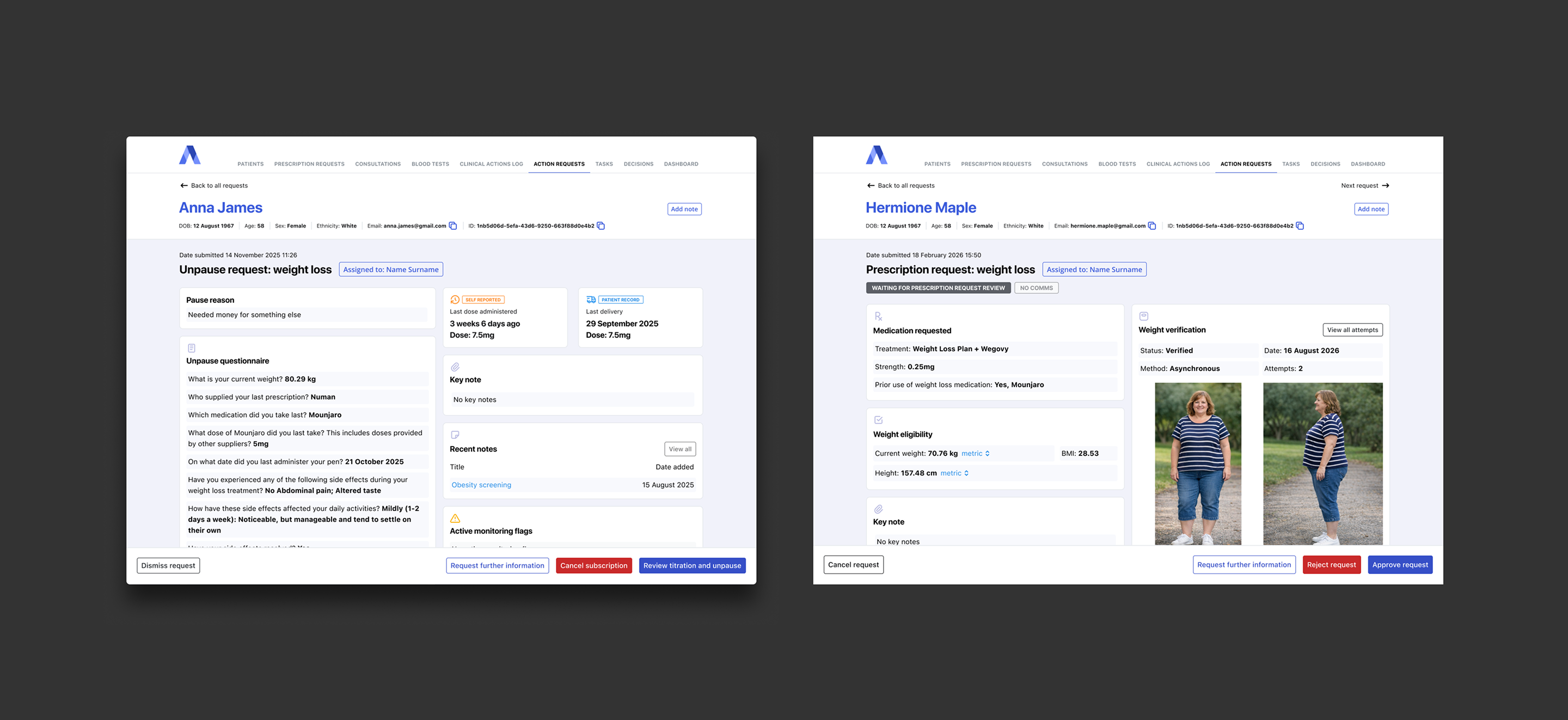
The design itself
To test ideas properly I needed prototypes built with realistic clinical data because clinicians pay close attention to detail and placeholder data would have given me surface-level feedback. Building out realistic patient scenarios took significant time and at points made me question whether the effort was proportionate. It was. When we went into testing, clinicians were scrutinising the smallest differences in patient data, and that level of engagement gave us genuinely useful signal.
Low fidelity ideas were tested early, and even at that stage clinicians immediately understood the value of what we were building - which was encouraging given how unfamiliar the interface was. Iterations informed the scope of v1, and high fidelity testing shaped v2. After introducing the new unpause request flow, the Customer Effort Score for that task improved from 3.4 to 4.1 out of 5 - a result that felt like a clear signal that the work was making a real difference.